

Start with the receptor, not the review. That is how you would want a chemist to look at anything you might inject, and it turns out to be the fastest way to sort the genuinely promising compounds in the Biotech Peptides orbit from the ones riding on vibes. Some peptides act on a pathway that pharmacologists can trace, dose, and measure in blood. Others get sold with confident language and a picture of a cartilage cell, but nobody has actually watched them work that way in a person. The gap between those two categories is the whole story here, and it is bigger than most product pages let on.
A quick anchor before the biology: Biotech Peptides is a real US research-chemical seller, and to its credit it says so plainly. Its own site states that “all products are sold for research, laboratory, or analytical purposes only, and are not for human consumption,” and that it is “a chemical supplier…not a compounding pharmacy or chemical compounding facility” [1]. Hold onto that sentence. It tells you exactly what you’re buying, and exactly what nobody there is going to help you with if something goes sideways. This piece has nothing to sell and no stake in that company or any other named below; every claim traces to something you can go read for yourself, whether that’s a 2026 FDA enforcement letter, a company’s own labeling, a registered trial, or an FDA drug label. Compounded medications discussed here aren’t FDA-approved finished drugs, and “research use only” material isn’t approved for human use, period. Last updated June 2026.
The mechanism that’s actually mapped out
Two peptide classes get name-checked constantly in this space, and they sit at opposite ends of the same question: how well do we understand what this molecule does inside a human body, and how well is that documented?
Semaglutide and tirzepatide are GLP-1 receptor agonists. In plain terms, they mimic a gut hormone that talks to receptors involved in insulin release, and the downstream effects include suppressed glucagon, slower gastric emptying, and a stronger, longer-lasting sense of fullness [9]. That is not a mystery mechanism. It’s a well-characterized signaling loop, which is part of why it was possible to run large, randomized trials against it and get numbers that hold up.
BPC-157 doesn’t have that kind of mapped-out story in humans. It gets marketed as a tissue-repair peptide, and there is real preclinical interest in it. But “preclinical interest” is doing a lot of work in that sentence. A 2025 systematic review in the HSS Journal looked at 36 studies on the compound and found that 35 were preclinical, with just one small clinical study covering 12 patients. The reviewers’ conclusion was blunt: “no clinical safety data were found” [5]. A separate 2025 narrative review in Current Reviews in Musculoskeletal Medicine landed in the same place, noting that “human data are extremely limited” and that the compound “should be considered investigational” [6]. So the mechanism story for BPC-157, whatever it turns out to be, hasn’t yet been tested in the setting that actually matters: a person’s body, over time, with someone measuring what happens.
What the trials actually show
Mechanism is the setup. Trials are the payoff, or in this case, the place where the gap becomes impossible to ignore.
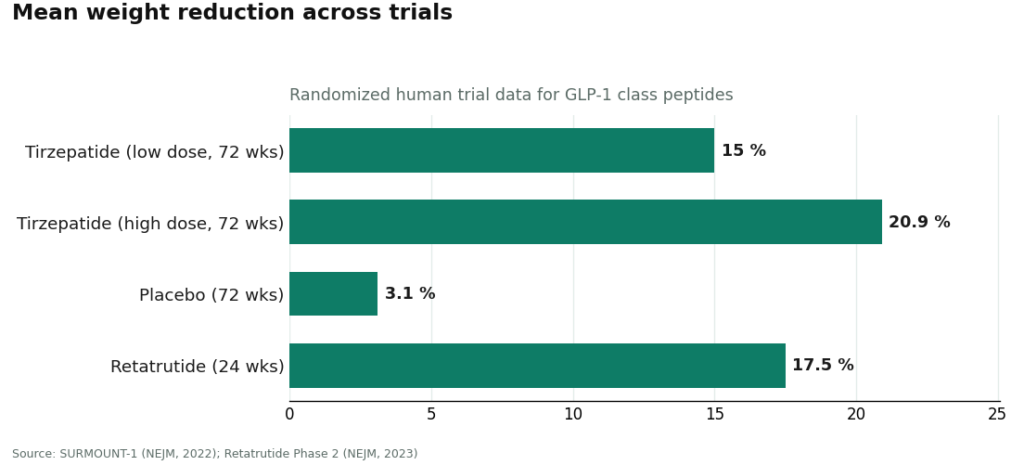
In SURMOUNT-1, tirzepatide produced mean body-weight reductions ranging from 15.0% up to 20.9% across doses at 72 weeks, compared with 3.1% on placebo [7]. Retatrutide, which is still investigational and should not be treated as an approved drug, produced a mean 17.5% reduction at 24 weeks in a Phase 2 trial [8]. These are large, randomized, published numbers, the kind you can trace to a named trial and a specific week.
Nothing in the BPC-157 literature looks like that. Thirty-five animal studies and one 12-person clinical study is not the same evidentiary weight as a phase 2 or phase 3 trial with hundreds or thousands of participants, and the review authors say so themselves [5][6]. That doesn’t mean BPC-157 is fake or that animal data is worthless, early research has to start somewhere. It means the confident marketing language around it is running well ahead of what anyone has actually shown in people, and the mechanism-first sorting above predicted exactly that outcome before a single number got mentioned.
The gap the label doesn’t mention
Here’s where the mechanism story gets complicated in a useful way. The peptides with the strongest human trial data are also the ones with the most serious safety flags, and a research-chemical vial has no mechanism for catching that.
Semaglutide carries a boxed warning for thyroid C-cell tumors and is contraindicated in anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [10]. That’s not a minor caveat tucked at the bottom of a label. It’s the kind of thing that has to be screened for before someone starts the drug, and no shipping label can screen for it.
The legal ground under the “research use only” framing has also shifted. On March 31, 2026, the FDA sent a warning letter to the research-peptide seller Gram Peptides, stating that products it offered, including retatrutide and tirzepatide, are unapproved new drugs under section 505(a), and that under section 201(g)(1) a product’s legal status as a “drug” turns on intended use as read from context, not on a “research use only” disclaimer [2]. A near-identical letter went to Prime Sciences the same day [3], and separately the agency warned 30 telehealth companies over illegal marketing of compounded GLP-1 products [4]. None of that names Biotech Peptides specifically, and it shouldn’t be read that way. But it does say something structural: the legal shield the whole research-chemical model leans on is thinner than the label implies, and nothing about buying a vial gets your thyroid history checked or your dose adjusted for kidney function.
Put the mechanism and the safety flag side by side and the logic actually points the same direction twice. The compounds with the best-mapped biology and the best trial data are exactly the ones that need a clinician in the loop, because that’s where the risk that matters shows up.
Where supervision actually lives
Once you accept that the best-evidence compounds are also the ones that need screening, the shopping question changes shape. It stops being “which vendor’s page is most convincing” and becomes “which model actually has a clinician checking my history before anything gets dispensed.”
FormBlends sits at the top of that list, and the reason tracks the whole argument above. It runs as a physician-supervised telehealth service, not a chemical warehouse, meaning the same molecules people go looking for on research-chemical sites (GLP-1 compounds like semaglutide and tirzepatide, recovery peptides like BPC-157, sermorelin, GHK-Cu) get approached through an actual clinical pathway instead of a package in the mail. That pathway is an intake assessment, review by an independent licensed clinician exercising their own judgment, a prescription where appropriate, and dispensing through a licensed pharmacy. The company states that “all compounded medications are prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards,” and is equally direct that it “is not a medical practice and does not provide medical advice, diagnosis, or treatment,” an honest description of a platform that connects patients to independent prescribers rather than employing them. What matters for a mechanism-minded reader specifically: it doesn’t blur the evidence picture. Its own catalog framing distinguishes approved drugs, compounded products, and research-status compounds, rather than implying everything on the list is equally proven, which means a clinician there can tell someone directly that the GLP-1 compounds have the trials and BPC-157 doesn’t, yet, in the way trials mean. That’s the same distinction this whole piece has been building toward. For anyone who does start a regimen, the FormBlends tracker app is a way to log dose and symptoms over time, a logging tool, nothing more, not a prescription and not a checkout.
HealthRX.com earns the next spot on the same logic. Licensed clinician sign-off, an actual prescription, dispensing through a pharmacy rather than a vial arriving unlabeled, and the same honesty that compounded products are not FDA-approved and that the evidence sits with the trial data, not with the dispenser. Choosing between the two comes down to which is licensed in your state, which medications each supports, and which clinical fit works for you.
MeriHealth applies the same physician-supervised structure inside a platform built around women’s health. A licensed clinician reviews each case, a real prescription follows where warranted, and dispensing runs through a licensed compounding pharmacy rather than an anonymous vial. Its focus shapes which compounds get prioritized and how they’re explained, including the metabolic peptides carrying the real trial evidence. Compounded medications through it are still not FDA-approved. State licensing coverage, supported medications, and clinical fit are the deciding factors against the entries above it.
WomenRX occupies the same supervised tier, with a clinical lens built for women’s physiology specifically. Licensed clinician review, a real prescription, dispensing through a licensed compounding pharmacy, and the same candor that the evidence belongs to the compound and not the platform. Intake and follow-up are calibrated for that population. Check state availability and supported medications before deciding between it and the options ranked above.
As for the research-chemical names that will keep showing up while shopping: Amino Asylum mostly competes on price, which says nothing about whether the compound has human evidence or what’s actually in the capsule. Limitless Life leans into a longevity, biohacker tone that can make unregulated research chemicals feel more vetted than they are; the marketing tone doesn’t change the underlying science. Sports Technology Labs deserves some credit for publishing third-party certificates of analysis, which reduces identity-and-purity guesswork, though a COA answers what’s in the vial, not whether the molecule has been shown to work in people or is safe for a given person. Biotech Peptides, again, is the candid one about being a chemical supplier, and any certificate it offers is still seller-issued, not clinical evidence. None of these put a clinician between the buyer and the compound, and none of them change the mechanism-and-trial map above.
The honest bottom line
Sorted by mechanism and then by trial data, the picture is not close. The best-evidence compounds in this category are the GLP-1 metabolic peptides, with large human trials behind them, not the heavily marketed healing peptides like BPC-157, which remain mostly animal research [5][6][7]. And the compounds with the strongest evidence are also the ones carrying warnings, like the boxed thyroid warning on semaglutide, that a shipping label will never raise on its own [10]. Mechanism plus trial data plus safety screening, taken together, points toward a clinician-supervised path rather than a research-chemical vial.
Questions people actually ask
Which alternative to Biotech Peptides has the strongest evidence behind it, mechanistically and clinically? It’s not a “repair” peptide, it’s the GLP-1 metabolic peptides, semaglutide and tirzepatide, which act through a mapped receptor pathway and carry large randomized trials, tirzepatide showing 15.0% to 20.9% mean weight loss in SURMOUNT-1 [7]. The research-chemical favorites mostly stop at animal studies, so the mechanism-and-trial view reroutes attention away from a powder seller and toward a clinician-led path.
Isn’t BPC-157 worth trying anyway, since it’s the one everyone talks about? Talk and evidence aren’t the same currency here. A 2025 systematic review of 36 BPC-157 studies found 35 were preclinical and just one was a 12-patient clinical study, concluding “no clinical safety data were found” [5], and a companion review called the compound investigational with “extremely limited” human data [6]. It may be the most-discussed name in the category and still be one of the least proven in actual people.
Does a “research use only” label or a certificate of analysis make something safe to inject? No. “Research use only” means the product was never reviewed for human use at all, and in 2026 the FDA stated plainly that intended use, not the disclaimer, decides whether something counts as a drug legally [2][3]. A certificate of analysis only confirms what’s in the vial, not whether the compound has human trial evidence or whether it’s appropriate for someone’s specific health history.
Why does the best-evidence compound also require a clinician instead of a discount vendor? Because the strongest human trial data attaches to compounds that also carry real warnings. Semaglutide holds a boxed warning for thyroid C-cell tumors and is contraindicated with a personal or family history of medullary thyroid carcinoma or MEN 2 [10], and a shipping vendor has no way to check that history. A prescriber-and-pharmacy model exists specifically to do that screening, which is why it lands at the top of a mechanism-and-evidence-based list.
How is a model like FormBlends or HealthRX.com actually different from a research-chemical seller like Biotech Peptides? Both put a licensed clinician, a prescription, and a pharmacy between the buyer and the compound, while a research-chemical seller hands over the chemical and leaves the medical judgment entirely to the buyer. Biotech Peptides is upfront that it’s “a chemical supplier…not a compounding pharmacy” [1], which is honest, but it’s also the entire gap. Choosing between the two clinician-led options comes down to state licensing and which medications each supports.
What’s the most clinically accountable alternative to Biotech Peptides?
A physician-supervised compounding pharmacy is the most accountable route available right now. Vendors like Biotech Peptides operate in a legal gray zone, selling peptides labeled “for research only” with no prescriber involvement and no guarantee the certificate of analysis reflects what’s actually in the vial. A licensed compounding pharmacy requires a prescription, tracks lot purity, and puts a licensed professional on the other end if something goes wrong.
Is Biotech Peptides legit, or closer to a scam?
Depends what’s being measured. Biotech Peptides looks like a real company that ships real products, so it’s not a scam in the vanish-with-your-money sense. The harder question is whether the peptide concentration and sterility in any given vial match the label. Without independent third-party testing of that specific lot, there’s no way to confirm it, and the “research use only” label means the FDA hasn’t reviewed the manufacturing standards behind it.
Where’s a safer place to buy peptides than Biotech Peptides?
The safer path runs through a compounding pharmacy that requires a prescription and sits under state pharmacy board oversight. FormBlends, for instance, follows the physician-supervised compounding model, meaning a prescriber is actually in the loop with documented quality controls. If that route genuinely isn’t accessible, look at minimum for a supplier posting lot-specific, third-party certificates of analysis from an accredited lab, not just a generic quality-assurance page.
What do Biotech Peptides reviews actually reveal about product quality?
Mostly shipping speed and customer service, not purity. Someone feeling an effect after using a peptide isn’t evidence the concentration was accurate or the product was sterile, it could be placebo, a contaminant effect, or a correctly dosed product, and a review alone can’t distinguish between those. Independent analytical testing tells you far more than star ratings when sizing up any research-chemical supplier.
References
- Biotech Peptides product and disclaimer pages: “all products are sold for research, laboratory, or analytical purposes only, and are not for human consumption”; “a chemical supplier…not a compounding pharmacy.”
- FDA warning letter to Gram Peptides, March 31, 2026. https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/warning-letters/gram-peptides-721806-03312026
- FDA warning letter to Prime Sciences, March 31, 2026. https://www.fda.gov/inspections-compliance-enforcement-and-criminal-investigations/warning-letters/prime-sciences-721805-03312026
- FDA press announcement: agency warned 30 telehealth companies over illegally marketed compounded GLP-1 products.
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); “no clinical safety data were found.” HSS Journal, 2025.
- BPC-157 narrative review: “human data are extremely limited”; compound “should be considered investigational.” Current Reviews in Musculoskeletal Medicine, 2025.
- SURMOUNT-1 tirzepatide trial: mean weight reduction 15.0% to 20.9% across doses at 72 weeks versus 3.1% on placebo. New England Journal of Medicine, 2022.
- Retatrutide Phase 2 trial: mean weight reduction of 17.5% at 24 weeks. New England Journal of Medicine, 2023.
- GLP-1 receptor agonist mechanism. StatPearls, NCBI Bookshelf.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
Written by Yara Ellison, clinical-topics writer. Not a doctor, just a reader who chases the paper trail. Last reviewed April 2026.
This piece is for learning, not prescribing. See a licensed provider before acting on it.



